Microsurgery is a particularly high-risk, high-stakes specialty with little margin for error and training of microsurgeons to ensure the highest quality of care and to minimize patient safety concerns may be of vital importance. Consequently, demonstration of measurable performance is important in order to evaluate skill acquisition and apply targeted feedback to improve training.
From Lee, S. et al, Ann Plast Surg, 10.1097/00000637-198307000-00008 (1983).
An ideal microsurgery assessment tool should be able to deconstruct all the subskills of microsurgery, to assess them objectively and reliably, and to show a good correlation between this assessment and outcome.
In this project, we will focus on:
- Visuo-spatial ability, which relates to the capacity to understand and remember the spatial relations among objects or space. This ability is required in vessel-wall dissection, suture-placement, and knot-tightening. The placement and spacing of sutures require visuo-spatial awareness to avoid catching the back-wall and suture entanglement. Lastly, knot-tying and knot-tightening under the microscope is also done under vision rather than by feel.
- Dexterity, which is the basic prerequisite for a microsurgical procedure and it relates to hand steadiness, flow of movements, finesse of surgery, instrument handling and tissue handling. Steadiness, i.e. absence of tremor, is a prerequisite to handle micro-instruments comfortably. Dexterous tissue handling is of importance to minimize tissue damage, which translates to a reduced risk of vessel thrombosis
Approach
Microsurgical model and skills assessments
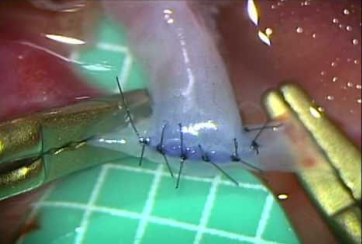
The participants will perform end-to-end anastomosis of chicken wing arteries using standardized microsurgical instruments and 9-0 monofilament sutures under microscopes. Each anastomosis will be assessed by two experts blinded to the participant’s identity.

From Hino A. Neurosurgery 2003;52(6):1495-1497.
During the procedure, we will use the subjective Stanford Microsurgery and Resident Training (SMART) scale to evaluate dexterity. It was created by microsurgical experts based on factors deemed important for technical performance and grades performance on a Likert scale from 1 to 5 of the following factors: instrument handling, tissue handling, suture handling, suturing technique, efficiency, quality of knot, operation flow, final product and overall performance.
Upon completion, each anastomosis will be cut longitudinally to view the intimal side and we will use the subjective ALI score to evaluate visuo-spatial ability. By opening the vessel at the end of the procedure and examining the regularity and structural architecture of the end product, Ghanem et al. were able to assess microsurgical skill through the identification of 10 errors that would lead to anastomotic failure such as leaking or thrombosis. Based on these 10 errors, an Anastomosis Lapse Index (ALI) was created and a pictorial representation of each error and a simple index to refer to the level of competency achieved was presented.
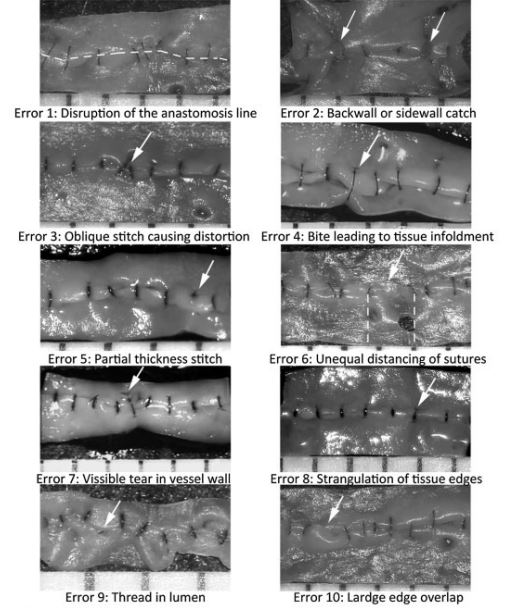
From Ghanem AM, et al. J Reconstr Microsurg. 2016;32(3):233-41.
Recording of motion, force and EMG activity
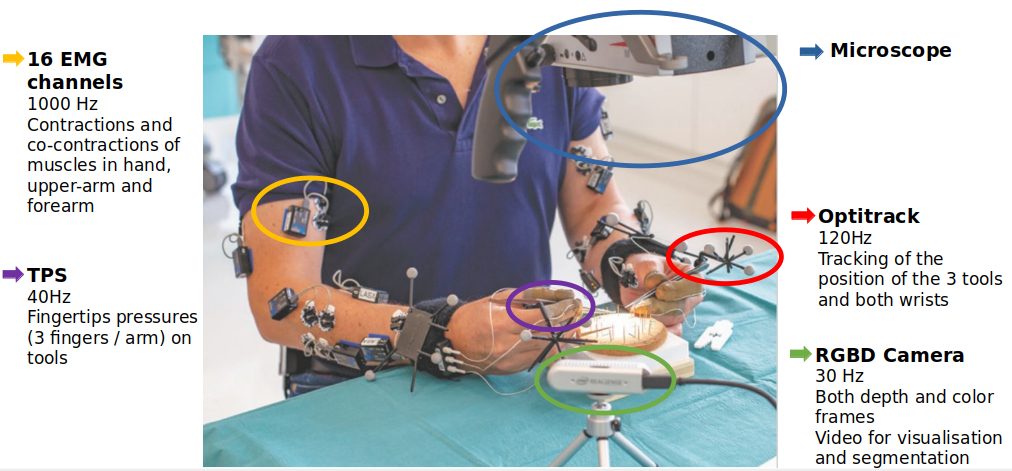
The participants will use microsurgical instruments with motion sensors and wear force sensors and muscle activity sensors. To study motion, we will use a high-resolution set of cameras tracking small markers mounted on the surgeons’ wrists and surgical tools.
We here opt to use Optitrack which offers high resolution tracking (360 frames per seconds and millimetric accuracy). We will use indirect information on the force produced by the surgeons like measurements of muscle contraction (by EMG) and the pressure applied on the tools. We hence seek to derive variations of forces generated during the surgical procedure.
The recording setup includes: an external RGBD camera which provided depth and color frames at 30Hz, used to segment manually the operation phases, an Optitrack set of cameras with markers, used to track precisely motion of hands and tools, EMG sensors on both arms (8 channels recorded at 1000Hz) and TPS fingertip pressure sensors, placed alongside the thumb, index and middle fingers.
Work plan
The study will be conducted in three steps, as delineated in the work plan below.

1. Recording and extracting features from motion, force and EMG activity
The first milestone will be devoted to conducting the first batch of recordings (motion, force and EMG activity) and to establish the data analysis for extraction of the features such as time, steadiness, fluidity, needle handling, learning curve.
2. Explaining data from optimal control theory to define the levels of expertise
The second milestone will be devoted to the analysis of the data in view of determining factors that best explain differences in skill between novices and experts and to define learning curves. A second batch of recordings will be conducted to add to the statistics of the first step.
3. A model to predict automatically skill levels
The third milestone will be devoted to test our findings against the hypotheses, validate the prediction model and learning curves, and to publish scientific articles.