The Reconfigurable Robotics Lab led by Prof. Jamie Paik has launched an action to develop potential assistive technological solutions for mitigating the COVID-19 Pandemic, which out-broke globally and in Switzerland.
EasyVent – Easy Built Emergency Ventilator
Medical ventilators are the critical equipment for providing artificial means of breathing to patients with severe respiratory complications, especially caused by COVID-19. Hospitals around the world have faced ever-increasing challenges of accommodating high number of patients with the limited equipment. In some extreme cases, doctors faced difficult moral choices between patients all desperately gasping for air. To address this problem, RRL’s action was toward the design and prototyping of an easy built ventilator, called EasyVent, equipped with minimum critical requirements. Similar efforts have been taken by many universities, including MIT, and many companies around the world. While such a solution is not meant to replace the existing clinically approved ICU ventilators, it could be vital in alleviating high machine demands for short term or in life-or-death situations with no other option.
We studied and characterized the ventilator performance for output tidal volume, pressure and respiratory rate using pressure and flow rate sensors.
System Overview
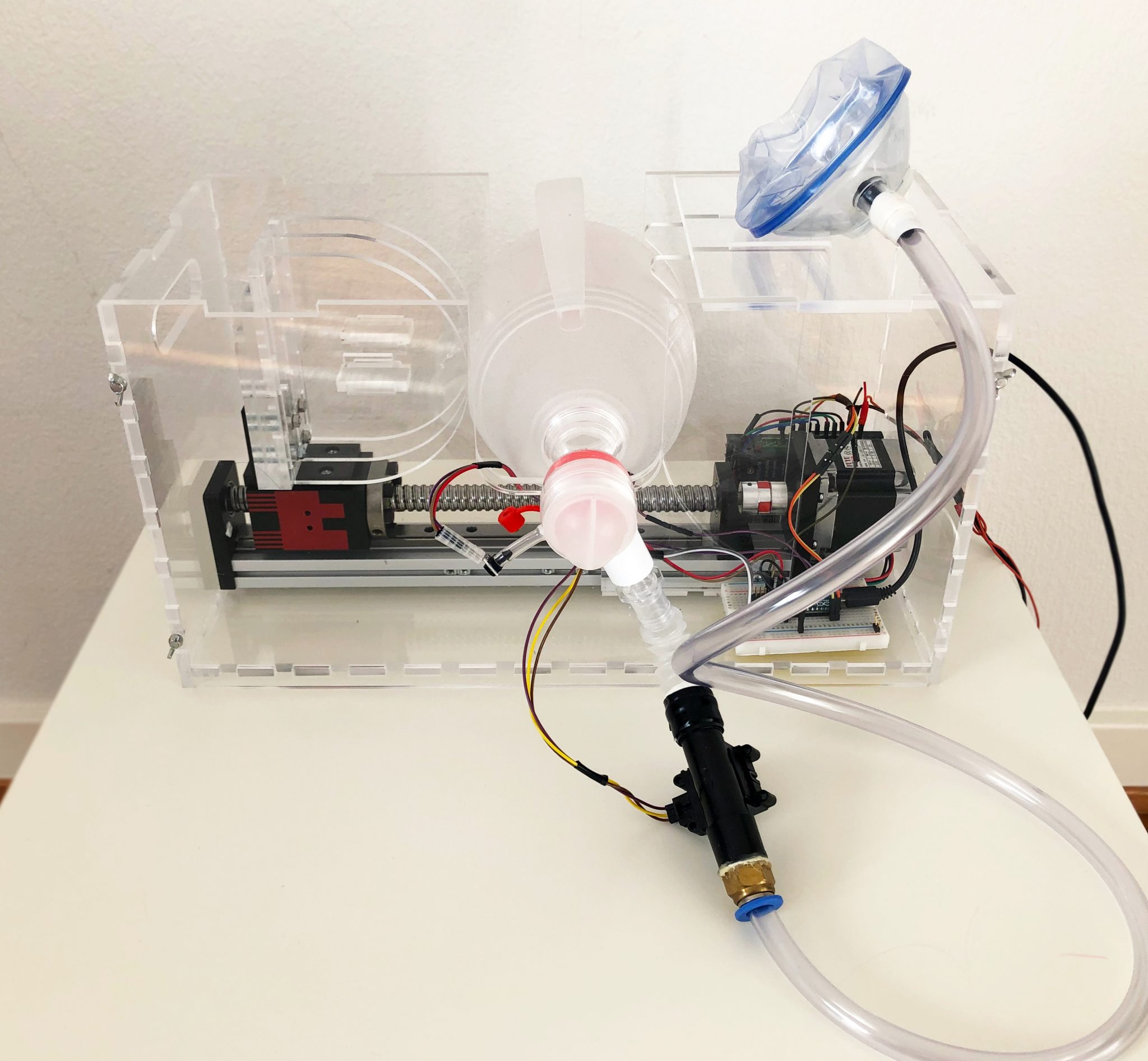
The ventilator system and essential components are depicted below. It comprise a medical grade manual resuscitator, Ambu bag, off-the-shelf linear stage mechanism, valves, flow and pressure sensors, Arduino micro controller and easy-to-assemble structural design adopted for automatic squeezing process of the resuscitator in programmed manner. Portable computer connected to the microcontroller allows monitoring and setting system parameters.
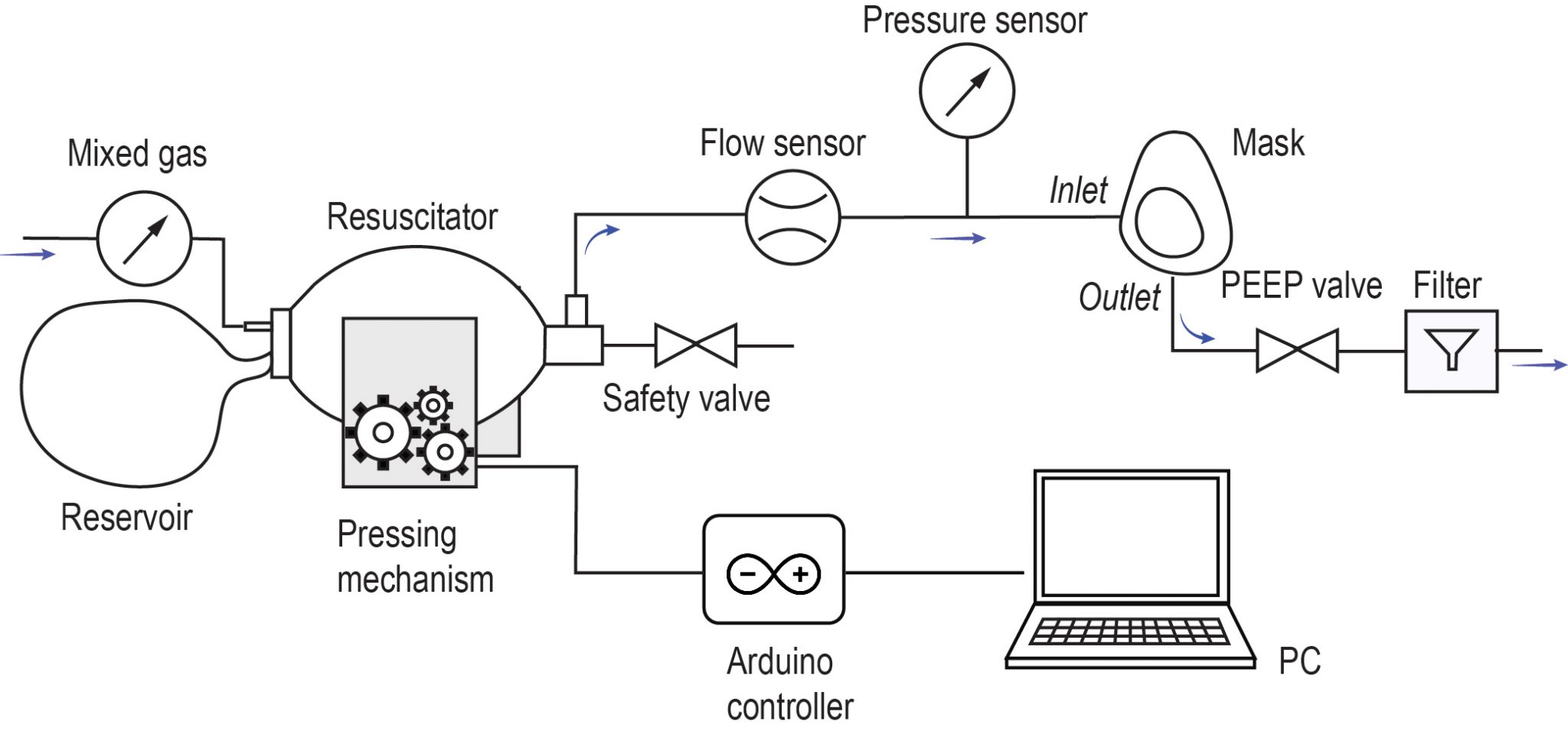
The pressing mechanism, driven by a stepper motor, compresses the Ambu bag to create air flow toward the mask for patient inspiration, while the expired air exhausts to the atmosphere through a positive end-expiratory pressure (PEEP) valve. PEEP valve keeps residual air in the lungs at the end of each breath by expanding alveolis, a balloon-shaped air sacs at the end of respiratory tree responsible for oxygen and carbon dioxide exchange to and from the bloodstream. This improves gas exchange and reduces lung trauma. Periodic press-inhale and release-exhale movements can be controlled by an algorithm running on a microcontroller and the setup allows for real-time measurement and parameter tuning.
Mechanical Design
For the ventilator pressing mechanism, we employ off-the-shelf linear stage mechanism (FSL40E200 05C7) to avoid mechanical imperfections and intolerance associated with custom made solutions. The readily assembled linear stage comprise a ball-screw coupled to a Nema 23 stepper motor. The motor rotates the lead screw clockwise or counter-clockwise, which then moves the stage back and forth, and its position can be controlled by adjusting the motor step size in open loop. The stage accommodates a convex-shaped “knuckle” structure that presses the Ambu bag against the stationary concave-shaped “bed” structure. Both elements are assembled from multiple layers of laser-cut 6 mm acrylic sheets, spatially distributed to produce three-dimensional structures. Such approach enables rapid cutting and fit-n-screw assembly process with minimal manufacturing steps.
Effectiveness of Snorkel Mask Sealing under Exhalation Air Pressure
Available ventilator solutions frequently use continuous positive airway pressure (CPAP) masks [1, 2] that are susceptible to leakage of COVID-19-contaminated aerosols into the ambient air [3]. This could potentially put the medical personnel at risk. To address this issue, RRL collaborated with the Laboratory for Bio- and Nano-Instrumentation (LBNI), headed by Prof. Georg Fantner, to study and characterize snorkeling masks as an alternative remedy to the leakage problem associated with CPAP masks.

Fig 1. (A) silicone covered 3D printed adult human face for realistic fit and compliance to human skin. (B) Actual snorkeling mask fitted on the whole head-assembly to replicate the real world wearing conditions. The straps were adjusted for optimal fitting. (C) Pressure sensor and flow sensor assembly.
The snorkeling masks are designed for usability under water where there is positive pressure outside the mask and relatively lower pressure (0 – 1 kPa). The most urgent measurement to be done is to determine whether the mask leaks when there is additional positive pressure in the mask, as is the case during ventilation.
Materials and Methods
To validate the effectiveness of the snorkeling mask, we decided to measure maximum positive pressure holding capacity of the mask and the leakage rate. If this capacity is comparable to the respiratory pressures, i.e. 1- 4 kPa (10-40 cm H20), we potentially can use the snorkeling mask to replace the CPAP and have improved protection against viral contamination.
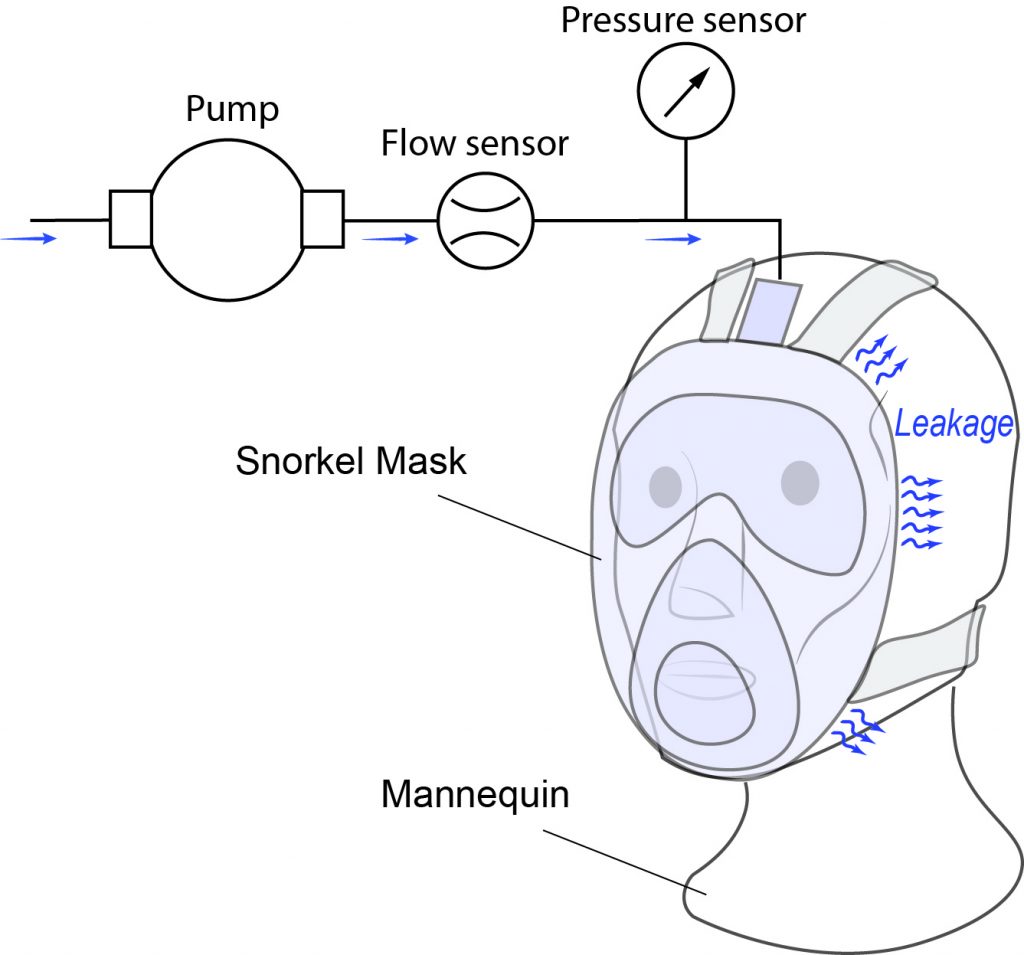
We designed a small test setup with a pressure sensor and flow sensor to measure the input pressure inside the chamber of the mask and amount of air flow inside (see figure below). In the ideal conditions where the mask is leak proof the flow rate should be zero and pressure of mask shall stabilize to the input applied pressure. The essential component of this testing is to have a human or human-like face to ensure optimal fitting on the face. We also paid special attention not to use any extra accessories to improve the fitting, the mask is as it came from the manufacturers; except a 3D printed connector from Snorkeling mask to 20 mm pneumatic outlet port [Consortium adaptateur-masque, France]. The test setup is devised for two measurement scenarios one with a standard size dummy human face and with a healthy human wearing the mask. We 3D printed an adult human dummy face and covered it with an approximately 5 mm thick coating of Dragon Skin 30 silicone (Smooth-on Inc.,USA) which is cured at 70°C for 30 mins. The silicone skin provides similar stiffness to the human skin in the range of 1 – 2 MPa.
Experimental Setup
A Honeywell pressure sensor with 0.1 kPa resolution and 0-100kPa range is connected to the entry port of the mask. Input flow of air is measured using a Honeywell flow sensor with 0-10 SLPM range. The input air is supplied through a 6 mm PVC tube connected to the pressure source with manually controlled input pressure ranging from 0- 4 kPa.
Results
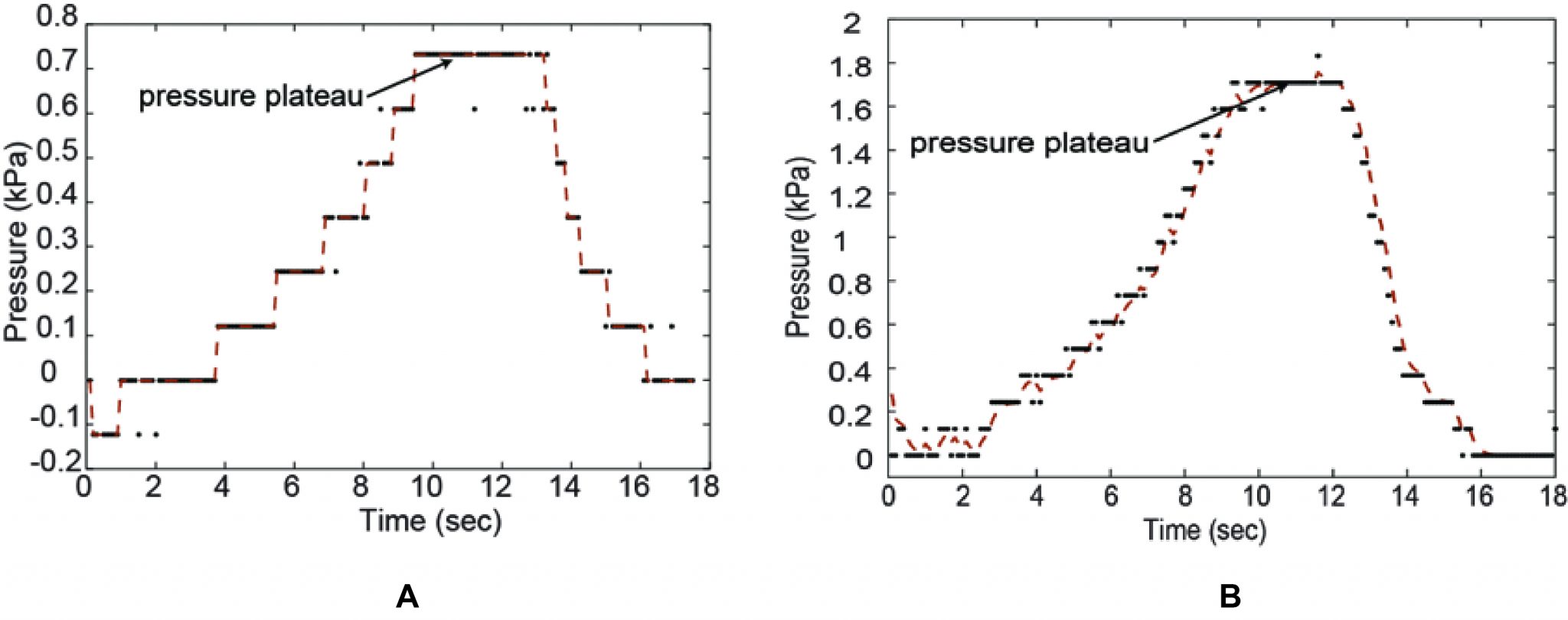
The experiment is conducted with a human face and a 3D printed soft silicone covered dummy face and the results are depicted in the figure below. In case of human face (A), we observed the input pressure inside the mask chamber rising from 0 to 0.9 kPa +/- 0.1 kPa and remains constant for applied pressure of 0 – 4 kPa from an external source. The extra volume of the air is leaked from the sides of the mask. Whereas, with 3D printed mask (B) the holding pressure inside the mask plateaued at 1.7 kPa +/- 0.1 kPa for 3 sets of measurements, one of which is as shown in Fig. 2.
Discussion and conclusion
While pressure increases, the mask progressively lifts away from the face (visual observation). Because the seal is not perfect, a small leak is visible. When the pressure becomes too high , the silicon skirt of the mask is no longer in contact with the skin of the test subject, and the air leak becomes so significant that the measured pressure no longer increases.
A maximum pressure of 0.7kPa (human test subject) – 1.7kPa (manikin head) can be applied in the mask. This range (0.7kPa-1.6kPa) is a reasonable estimate of the maximum pressure that could be applied if the decathlon mask was used for a CPAP system.
Acknowledgements: The work has been carried out in collaboration with RRL and LNBI laboratories at EPFL. Harshal Sonar, Zhenishbek Zhakypov, Mustafa Mete from RRL, and other Ph.D. candidates from LNBI conceptualized and designed the device. Harshal Sonar created the test setup and the silicone skin for the mask. Mélanie Hannebelle and Harshal Sonar conducted the tests. We are thankful for (UBO, France) and Santiago Andany for providing the 3D CAD model of the human head and 3D printing of this model head, respectively. Prof. Georg Fantner and Prof. Jamie Paik supervised the project and obtained the authorization for lab access.
References
[DS30] : “Dragon skin -30”, smooth-on Inc., http://www.smoothon.com/tb/files/DRAGON_SKIN_SERIES_TB.pdf
[1] World Health Organization (March 2020). COVID-19 v4. Retrieved from the link.
[2] World Health Organization (March 2020). Clinical management of severe acute respiratory infection (SARI) when COVID-19 disease is suspected. Retrieved from: https://www.who.int/docs/default-source/coronaviruse/clinical-management-of-novel-cov.pdf
[3] Wax, R.S., Christian, M.D. Practical recommendations for critical care and anesthesiology teams caring for novel coronavirus (2019-nCoV) patients. Can J Anesth/J Can Anesth (2020). https://doi.org/10.1007/s12630-020-01591-x